Clubfoot
Reid Nichols, M.D.
Introduction
Clubfoot is the most common deformity of the foot bones and joints in newborns. It occurs in about 1 in 1,000 babies. There are approximately 200,000 new clubfoot cases each year worldwide. Males are affected more than females (2:1). Children who are treated for a clubfoot or clubfeet may live full active lives. The goal is to start treatment in the first few weeks (1-2 if possible) after birth. About 98% of clubfeet respond to the Ponseti Method, which is the most commonly used method in North America.

Cause
The cause of clubfoot is not exactly known, but it most likely has a genetic component and in most cases is not caused by anything the parents did or did not do. Environmental factors such as smoking during pregnancy may be associated with clubfeet. Clubfoot is usually diagnosed on an ultrasound around the 20th week. The chances of having a second child with a clubfoot are approximately 1 in 30. When one parent is affected with clubfoot, there is a 3% to 4% chance that the offspring will also be affected. However, when both parents are affected, the offspring have a 30% chance of having a clubfoot.
Description
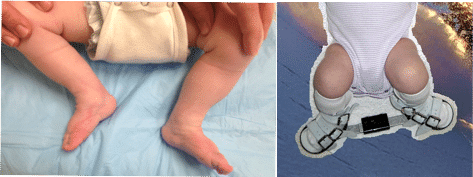
Clubfoot is a birth defect that causes one or both of a baby’s feet to turn inward and downward, giving the foot or feet a club-like appearance. If clubfoot only affects one side, the affected foot, calf, and leg may be smaller than the other side as the tissues of the lower leg and foot are affected.
Doctor’s Examination
Although 80% of babies with clubfoot have no other associated conditions, it can be related to other syndromes such as spina bifida or chromosomal abnormalities. The doctor will perform a head to toe evaluation.
Nonsurgical Treatment
The Ponseti Method is a surgery minimizing technique which is comprised of two phases. During the first phase, the foot is gently manipulated and placed in a cast up to the mid thigh every four to seven days during a 3-to-8 week period. Most clubfoot deformities can be corrected in approximately 6 weeks. The foot slowly moves into the right position with gentle stretching and casting. Treating early takes advantage of the elasticity or stretchiness of the ligaments and joints of an infant’s foot. A small surgery to release the tight heel cord is commonly performed between the last two casts. The second phase of treatment is the bracing phase which may last between 2 and 5 years as the foot grows most rapidly. In the first three months the brace is worn full-time and then just at night. The Ponseti brace is essential to preventing relapse or need for further surgery.
There is a separate approach called the French method which realigns the foot with stretching and taping. The advantage is that casts are avoided, while the disadvantages are that daily specialized care is necessary for months and more severe deformities are difficult to treat with the French method.
Surgical Treatment
Although even the most challenging clubfeet often respond well to casting if treated early, many patients will need surgery. The most common procedure is called a tibialis anterior tendon transfer, which helps balance out the movement of the foot.
Some children will have recurrence of the clubfoot deformity. They often are plump feet with stiff ligaments and a deep crease in the bottom of the foot. There are many options including soft tissue procedures to release tight ligaments and bony cuts to reshape the foot. A very small percentage of children have such severe deformity that even these more invasive surgeries are not successful. In these cases, an external fixator can be very helpful. This is a metal frame connected to the foot by pins and wires, which allows for gradual correction of the foot. In younger children the correction is performed by stretching through the joints, while in older children the correction is performed by cutting the bones and then reshaping them with the external fixator.
Adults do not respond to casting and need surgery if basic shoe inserts are inadequate. In adults the rigidity of the foot requires an external fixator to gradually restore foot alignment. Tendon transfers may be helpful to balance the foot and prevent recurrence of the clubfoot deformity. As in children, bracing after surgery is critical to maintaining the proper foot position.